What is a Discectomy?
A discectomy is a type of spine surgery used to remove part of a spinal disc that is damaged and pressing on nearby nerves. Spinal discs act as cushions between the bones (vertebrae) of the spine. When a disc becomes herniated, slipped, or ruptured, it can bulge out and compress the spinal nerves.
This pressure often leads to symptoms such as:
- Persistent back or neck pain
- Pain radiating into the arms or legs (sciatica is a common example)
- Numbness or tingling in the hands or feet
- Muscle weakness that affects walking, gripping, or daily activities
The main goal of a discectomy is to relieve pressure on the nerves, reduce pain, and restore normal movement and function. It is usually recommended only when medications, physical therapy, and other non-surgical treatments fail to provide relief.
Types of Discectomy
Discectomy procedures vary depending on the location of the disc problem, the severity of nerve compression, and the surgical method chosen. Each type has its own benefits, risks, and recovery expectations.
Lumbar Discectomy
- Where it is done: Lower back (lumbar spine).
- Why it is done: To relieve pain, tingling, or weakness in the legs caused by a herniated or slipped disc pressing on the spinal nerves (often called sciatica).
- Key points: This is the most common form of discectomy because lumbar disc herniations occur more frequently than in other spinal areas. Patients usually notice significant relief in leg pain soon after surgery.
Cervical Discectomy
- Where it is done: Neck region (cervical spine).
- Why it is done: To ease symptoms such as arm pain, numbness, weakness, or difficulty with hand coordination caused by nerve compression.
- Special note: Surgeons often combine this with spinal fusion or artificial disc replacement to restore stability and prevent abnormal motion in the neck.
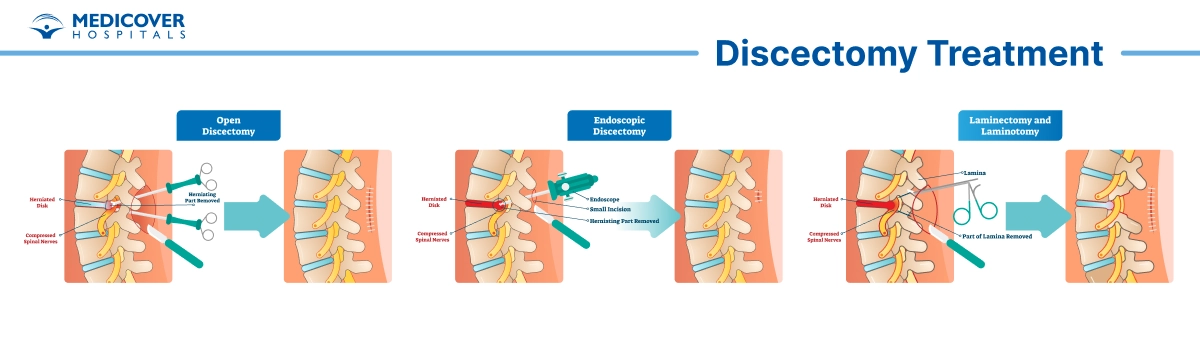
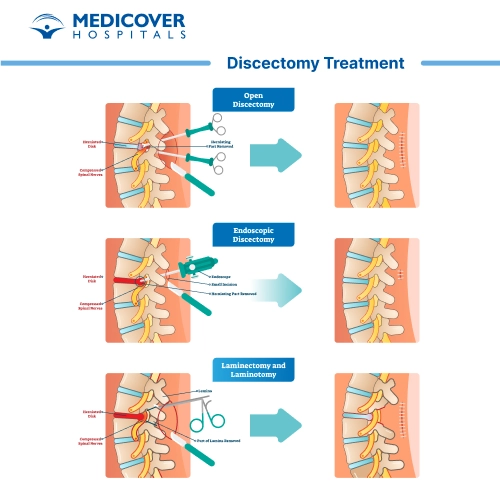
Open Discectomy
- Method: A standard surgical technique where the surgeon makes a small incision in the back.
- Process: Muscles and tissues are carefully moved aside to reach the affected disc. The damaged portion pressing on the nerve is removed.
- When used: Often recommended when the herniation is large, when minimally invasive options are not suitable, or when previous surgeries have failed.
Microdiscectomy (Microscopic Discectomy)
- Method: A minimally invasive procedure using a surgical microscope for better precision.
- Advantages:
- Smaller incision (usually 1-2 cm).
- Less muscle and tissue disruption.
- Faster healing and shorter hospital stay.
- Who benefits: Patients with severe leg pain from lumbar disc herniation are the best candidates.
Microendoscopic Discectomy
- Method: Uses an endoscope (a thin tube with a camera) and specialized surgical tools.
- Advantages:
- Even less disruption to muscles compared to microdiscectomy.
- Reduced scarring and blood loss.
- Shorter recovery time and quicker return to daily activities.
- Consideration: Requires advanced surgical expertise and may not be available in all hospitals.
Laminectomy vs. Discectomy
- Laminectomy: Removes part of the vertebral bone called the lamina. This creates space to relieve pressure on the spinal cord or nerves.
- Discectomy: Removes the herniated or damaged disc material that is pressing directly on a nerve.
Combination approach: Sometimes both procedures are done together if bone and disc material are contributing to the nerve compression.
1-2 Hours
Surgery Duration
General Anesthesia
Anesthesia Used
2-3 Weeks
Full Recovery Timeline

When is Discectomy Recommended?
A discectomy is usually considered when other treatments like rest, medicines, or physiotherapy do not bring enough relief. Doctors carefully evaluate the symptoms, MRI scans, and overall health before suggesting surgery.
Common Situations Where Discectomy May Be Needed:
Persistent Leg or Back Pain
- If severe pain continues for several weeks or months despite non-surgical treatments, surgery may be suggested.
- Pain often radiates down the leg (sciatica), making it hard to sit, walk, or sleep comfortably.
Herniated or Slipped Disc Pressing on Nerves
- A disc that bulges or slips out of place can press on nearby spinal nerves.
- This pressure may cause sharp, shooting pain, especially in the lower back or legs.
Numbness, Weakness, or Tingling in Limbs
- When a nerve is compressed, it can affect muscle strength and sensation.
- Patients may feel weakness in the legs, difficulty lifting the foot (foot drop), or a constant tingling sensation.
Loss of Bladder or Bowel Control (Emergency)
- This is a rare but serious condition known as cauda equina syndrome.
- It needs urgent surgery to release pressure on the nerves and prevent permanent damage.
How to Prepare for Discectomy Surgery?
Good preparation makes the surgery smoother and recovery easier. Patients and caregivers should plan ahead, both medically and at home, to reduce risks and support healing.
Medical Evaluation and Tests
Before surgery, doctors perform a detailed evaluation to confirm the need for a discectomy. This may include:
- Blood tests: to check for infection, anemia, or clotting problems.
- X-rays: to look at spinal alignment and bone condition.
- MRI or CT scans: to pinpoint disc herniation and pressure on nerves.
- Physical examination: to assess pain, strength, and mobility.
These tests help the surgical team decide the safest and most effective approach.
Lifestyle Adjustments
Certain habits can slow healing or increase risks. Patients are usually advised to:
- Stop smoking: Smoking reduces oxygen supply to tissues and delays recovery.
- Avoid alcohol: Alcohol can interfere with anesthesia and post-surgery medicines.
- Discontinue blood-thinning medicines: Drugs like aspirin, ibuprofen, or warfarin may increase bleeding risk. Your doctor will guide you on when to stop and restart them.
- Maintain healthy activity: Gentle exercise, like walking, can improve strength before surgery.
Home Preparation
Making your home recovery-friendly is an important step:
- Arrange assistance: Ask a family member or friend to help with meals, errands, and daily activities for the first few days.
- Set up a recovery area: Prepare a bed or chair that supports your back and allows easy movement.
- Keep essentials nearby: Place water, snacks, phone, medications, and remote controls within reach to avoid bending or stretching.
- Remove hazards: Clear walkways and secure rugs to reduce fall risks.
The Day Before and Day of Surgery
Following hospital instructions helps prevent complications:
- Fasting: Do not eat or drink for 6-12 hours before surgery, as advised.
- Bathing: Use antiseptic soap or follow hospital instructions to reduce infection risk.
- Clothing: Wear loose, comfortable clothes and remove jewelry or accessories.
- Documentation: Carry your ID, insurance papers, and medical records.
What Happens During Discectomy Procedure?
Discectomy removes the part of a spinal disc that presses on a nerve.
The goal is simple: take the pressure off the nerve so pain eases and strength returns.
Quick Overview
- Anesthesia: General anesthesia. You sleep through the surgery.
- Incision: Small cut in the back or neck, based on the disc level.
- Main Step: The surgeon removes the disc fragment that hits the nerve.
- Closure: The cut is closed with stitches or staples.
- Recovery: You wake in recovery, then move to a ward or go home the same day.
Before the Operation (Same Day)
- Check-in: Nurses confirm your name, procedure, and side/level.
- IV line: A small tube goes into a vein for fluids and medicines.
- Marking and review: The surgeon reviews the plan and answers last questions.
- Antibiotic dose: Given to lower infection risk.
- Anesthesia start: You breathe oxygen, then go to sleep.
In the Operating Room-Step by Step
Positioning
- You lie face down on a padded frame (for lumbar) or face up for some neck cases.
- Soft pads protect your eyes, hips, knees, and elbows.
- A warming blanket helps keep body temperature normal.
Imaging and Level Check
- The team uses X-ray (fluoroscopy) to confirm the exact disc level.
- A safety pause ("time out") confirms patient, procedure, and level.
Incision / Access
- The skin is cleaned with antiseptic.
- A small incision (often 2-5 cm) is made over the target level.
- Muscles are gently moved aside, not cut, to reach the spine.
- A microscope or loupes may be used for a clear, precise view.
Tiny Bone Window (If Needed)
- A very small part of bone (lamina) may be shaved (laminotomy).
- This creates space to see the nerve and disc safely.
Nerve Protection
- The nerve root is identified and gently protected with soft retractors.
- The surgeon checks for tight bands or small spurs that add pressure.
Disc Fragment Removal (Discectomy)
- The herniated disc piece is removed with fine tools.
- Only the part causing pressure is taken out; the healthy disc is left in place.
- The surgeon checks the space to be sure the nerve moves freely.
Final Checks and Closure
- The area is rinsed and bleeding points are sealed.
- The muscle and skin are closed in layers.
- A small dressing covers the incision.
After Surgery (Recovery Room)
- Monitoring: Heart rate, blood pressure, and oxygen are watched closely.
- Comfort: You get pain and anti-nausea medicine as needed.
- Movement: Nurses help you sit, stand, and walk when safe.
- Eating/Drinking: You start with sips, then light food.
- Discharge: Many people go home the same day; some stay one night.
What to Expect After Discectomy Procedure?
Most people get fast relief of leg pain after a discectomy and then recover gradually over weeks to months.
First few hours - first few days
- You wake in a recovery room. Nurses watch your pain, breathing and the wound. You may go home the same day or stay 1-2 days if needed.
- Pain and stiffness are normal. Expect soreness near the incision and some nerve-type pain (tingling, numbness) that may take longer to improve.
- Move early. Short, frequent walks are encouraged from day one. Walking lowers risks (blood clots, stiffness) and speeds recovery.
- Medicines: your team will give pain drugs. Short courses of opioids may be used at first. You will usually switch to acetaminophen or an NSAID and, if needed, a nerve pain medicine (for burning or tingling).
- Bowel care: opioid pain meds and less activity can cause constipation. Drink fluids, eat fiber, and use stool softeners if advised.
Weeks 1-4 (early recovery)
- Walking and light daily tasks increase each day. Do many short walks rather than one long sit.
- Wound care and showering: most teams let you shower after 48-72 hours. Keep the incision from being soaked (no baths or pools) until your surgeon says it's healed. Follow the exact dressing and shower rules on your discharge sheet.
- Avoid heavy lifting, deep bending, or twisting (often called BLT) for about 3-6 weeks. Do not carry heavy loads.
- Driving: don't drive while taking sedating pain meds. Many patients can drive again when they can sit comfortably, react normally, and do an emergency stop - commonly around 2-6 weeks. Check with your surgeon and your insurance.
Weeks 5-12 (gaining strength & return to work)
- Light office work is often possible by 4-6 weeks. Heavy manual work may need 3 months or more. Timelines vary with the job and how you heal.
- Physical therapy (PT): many surgeons start structured PT within 4-8 weeks. PT focuses on gentle walking progressions, posture, core strength, and safe body mechanics.
- Expect gradual return of strength and less nerve pain over weeks. Nerves heal slowly sensations and weakness can improve for months.
3-6 months and beyond (full recovery and outlook)
- Many people reach near-full function by 3-6 months. Some symptoms (numbness, weakness) may take longer to improve. In some cases patients report continued gains up to a year or more. Follow-up visits track progress.
- Long-term goals: normal walking, return to work and hobbies, good pain control, and stronger core and back support.
Wound and home care - practical do's & don'ts
- Keep dressings as instructed. Do not soak the wound. Let water run over it in the shower and pat dry.
- Watch for signs of infection: spreading redness, new or increasing drainage, rising fever, or opening of the wound. Call your surgeon if these appear.
- No swimming, hot tubs or baths until the wound is fully healed (usually several weeks).
Benefits of Discectomy Surgery
A discectomy can greatly improve the quality of life for people suffering from a herniated or slipped disc. Some of the key benefits include:
- Pain Relief: The surgery removes the part of the disc pressing on the nerve, which reduces or completely relieves back and leg pain.
- Better Mobility: With reduced pain, patients can move more freely, sit, walk, and even exercise without constant discomfort.
- Faster Recovery: When conservative treatments like medicines, injections, or physical therapy fail, surgery often provides quicker and longer-lasting results.
- Prevention of Nerve Damage: Untreated disc problems can lead to permanent nerve damage, weakness, or numbness. Surgery helps prevent such long-term complications.
- Improved Quality of Life: By reducing pain and restoring movement, patients can return to work, hobbies, and daily activities more comfortably.
Risks of Discectomy Surgery
While discectomy is considered safe, every surgery carries some risks. Fortunately, these complications are rare and most patients recover well. Possible risks include:
- Infection: A small risk of infection at the surgical site, which can be managed with antibiotics.
- Bleeding or Nerve Damage: Minimal blood loss is common, but in rare cases, nerves near the spine may be injured.
- Recurrence of Disc Herniation: The same disc, or another disc, may slip again in the future, though this happens in only a small percentage of patients.
- Anesthesia-Related Risks: Some patients may experience reactions to general anesthesia, but this is closely monitored by specialists.
What is the Cost of Discectomy in India?
The cost of discectomy varies depending on the complexity, surgeon's expertise, and hospital facilities. On average, it ranges between Rs. 80,000 to Rs. 3,20,000. To know the exact cost for your case, please contact our customer support team for detailed guidance.