Contributors

Dr. Ramavath Dev
Chief Consultant - Hemato & Medical Oncology

Dr. D S K Sahitya
Consultant Clinical Hematology & BMT
A 14yr old girl presented with chief complaints of menorrhagia, skin and gum bleeds along with shortness of breath on exertion. She reached out to a local pediatrician with the above complaints and is referred to our center for Hematologist opinion. On examination, she had severe pallor, petechiae and ecchymosis.
Her baseline investigations revealed Hb – 3.4gm/dl (MCV – 102), TLC – 2600 (N – 22%, L -73%, E-4%, M-1%), Platelet Count – 12,000 and a reticulocyte count - 0.5%. Peripheral smear showed anisopoikilocytosis, marked leucopenia and thrombocytopenia.
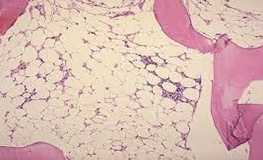
Further investigations revealed, bone marrow aspirate and biopsy showed hypocellular marrow (10%- 20%) with reduced trilineage hematopoiesis. Normal Chromosomal breakage study was done to rule out any genetic etiology. Paroxysmal Nocturnal Hemoglobinuria(PNH) clone was found on 59% of neutrophils and monocytes by flow cytometry. With all the workup, she was diagnosed with severe Aplastic Anemia.
Next, we have done a Human Leucocyte Antigen (HLA) typing with her younger sister which revealed a 12/12 full match. After extensive counselling to the family, we took the patient for allogenic matched sibling bone marrow transplant. She received conditioning with Fludarabine, Cyclophosphamide and Horse anti-thymocyte Globulin followed by stem cell infusion. She engrafted on day 12 of transplant. There were no major complications in the peri transplant period. She is on cyclosporine for graft versus host disease(GVHD) prophylaxis along with antimicrobial prophylaxis. Currently, she is on day 36 post-transplant and is doing well.
Chromosomal breakage study was done to rule out genetic causes was normal. Based on the above investigations, she was diagnosed with severe aplastic anemia

Chief Consultant - Hemato & Medical Oncology
Consultant Clinical Hematology & BMT
Feeling unwell?
Book Doctor Appointment in 30 Sec