Retroperitoneal Mass at Medicover
Nov 04 2022 | Medicover Hospitals | KakinadaA 55-year-old female came to Medicover Kakinada. with gross abdominal distension and breathlessness due to mechanical effect of the distended abdomen. On enquiring further, she was diagnosed to have large abdominal mass of inconclusive origin 4 years ago and she had history of recurrent Supraventricular Tachycardia episodes and was on treatment with medicines.
In view of old age and frailness, very large abdominal complex cystic mass of inconclusive origin, cardiac arrythmia - surgical treatment was deferred by most hospitals. Patient and her attendants lost hope of cure and went for alternative medicine but tumor size increased further in size, caused mechanical pressure effects and nutritionally deprived her.
She was admitted and optimised nutritionally. Once patient got better symptomatically, she was reviewed again with all her old reports and imaging data. At the request of patient’s attendants, we proceeded with re-evaluation of mass for chance of operability. She was nutritionally compromised with severe malnutrition due to mechanical effects of tumor and tumor cachexia.
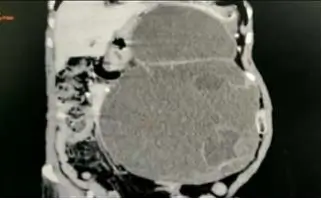
CECT abdomen with proper protocol performed, suggestive of large cystic mass of about 33x25 cm size which was extending from left dome of diaphragm to pelvis compressing all near-by structures and identified to be arising from distal body of pancreas probably mucinous cystadenoma of pancreas.
It was further confirmed by CA 19.9 - >1000.
After thorough evaluation – patient’s attendants were counselled about the possibility of resection. Explained very high risk of the procedure and the possible complications that can arise from such major surgeries. Patient attendants gave consent to proceed with surgery.