Calcified Lesions Surgery Hospital with Expert Care
Medicover Hospitals provides expert care for calcified lesions with experienced specialists and advanced diagnostic technology. We focus on early detection, accurate evaluation, and effective treatment planning. Our patient-centric approach ensures safe procedures, timely intervention, and better long-term outcomes through comprehensive care and continuous monitoring.
Expert Surgeons
Successful Surgeries
Success Rate
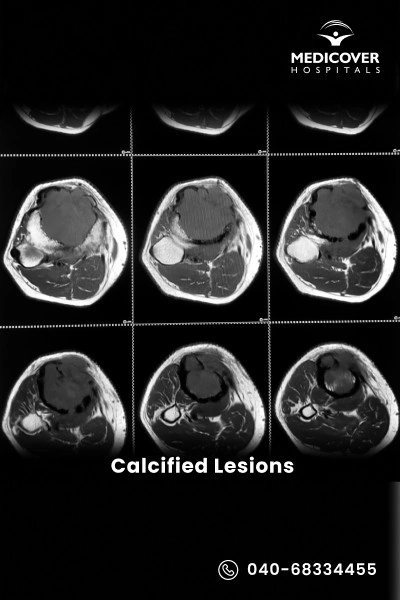
What is Calcified Lesions?
Calcified lesions, also known as calcifications, are abnormal calcium deposits that build up in tissues, blood vessels, organs, or even the brain. They are often detected through imaging tests like X-rays, CT scans, or MRIs. While some are harmless, others may result from chronic inflammation, injury, metabolic disorders, or circulatory problems, and can lead to pain, stiffness, or organ dysfunction depending on their size and location.
Types of Calcified Lesions
There are several types of calcification, each with its own characteristics:
- Vascular Calcifications
- Soft Tissue Calcifications
- Organ Calcifications
- Brain Calcifications
- Dystrophic Calcifications
- Metastatic Calcifications
Calcified Lesions Treatment Specialists Near You
Find expert doctors for calcified lesions treatment across India in multiple locations. Choose your city to connect with specialists for accurate diagnosis and advanced care.
Why Choose Medicover Hospitals for Calcified Lesions Treatment
Get a second opinion from trusted experts and makeconfident, informed decisions.
Complete Guide to Calcified Lesions Surgery
Everything you need to know about the procedure, preparation, and recovery
When Is Treatment Needed?
Not all calcified lesions require immediate care, but treatment becomes important in certain situations. The main indications of Calcified Lesions include cases where they cause pain, swelling, or limit movement.
Some other important indications of Calcified Lesions include:
- When linked to underlying health conditions such as infections, autoimmune disorders, vascular problems, or cancer.
- If the lesion shows rapid growth, changes in shape, or unusual patterns on scans.
- When calcifications interfere with vital organ function such as the brain, heart, kidneys, or lungs.
- If there is a risk of serious complications, like blockages in blood vessels.
- When a doctor recommends further investigation, biopsy, or removal for safety.
In short, treatment for calcified lesions is needed when they cause symptoms, impair organ function, or suggest a more serious underlying disease.
Preparation For Calcified Lesions Procedure
Proper preparation before your appointment ensures accurate diagnosis, effective communication with your doctor, and helps in choosing the best treatment plan for calcified lesions.
- Gather Medical Information: Collect your medical history, including past diagnoses, medications, surgeries, and family health history, to help you understand your overall health.
- List Symptoms and Concerns: Note down any symptoms you're experiencing and any questions or concerns about the calcified lesion for your appointments.
- Research Healthcare Providers: If you haven't been referred to a specialist, research doctors specializing in areas like orthopedics, cardiology, or dermatology for treatment of calcified lesions.
- Schedule Appointments: Make appointments with healthcare providers and ask your primary care doctor for referrals if needed.
- Write Down Questions: Prepare a list of questions to ask your doctor about the lesion, its causes, treatment options, and expected outcomes.
- Prepare Relevant Documents: Bring your medical records, test results, and imaging studies (like X-rays or MRIs) to your appointments for better assessment.
- Review Your Medications: List all the medications, supplements, and vitamins you're taking and share them with your doctor for a complete medical overview.
- Prepare for Diagnostic Tests: If tests like blood tests or imaging studies are needed, follow the instructions given by your healthcare provider, such as fasting or wearing suitable clothing.
- Ask About Treatment Options: Discuss treatment options with your doctor, including the risks, benefits, and expected results.
Procedure For Calcified Lesions Surgery
The management and treatment approach for calcified lesions depends on the underlying cause, the location of the calcifications, and the potential impact on the individual's health. Here are some common approaches used for calcified lesions:
- Diagnostic Assessment: If calcified lesions are found, further tests, including blood tests, biopsies or imaging, might be done to determine their cause and nature.
- Observation and Monitoring: For small, asymptomatic calcifications, physicians may also monitor over time with routine imaging to look for change.
- Lifestyle Changes: Making changes in your lifestyle like improving heart health and eliminating risk factors like high blood pressure and cholesterol can help with the management of certain types of calcifications.
- Medications: We can use medications to relieve symptoms, reduce inflammation, and prevent further calcifications, depending on the etiology.
- Physical Therapy and Rehabilitation: If calcifications affect soft tissues or joints, physical therapy can improve mobility, relieve pain, and prevent complications.
- Surgical Removal: Surgery may be needed if the calcifications cause discomfort or impair organ function, especially in more severe cases.
- Treatment of Underlying Conditions: Addressing the underlying cause, like an infection or inflammation, can help prevent further calcification.
Recovery After Calcified Lesions Surgery
Recovery varies depending on the type of treatment, but here's a general timeline:
First Few Days
- Rest and allow your body to heal.
- Manage pain with prescribed or over-the-counter medications.
- Follow wound care instructions if surgery was performed.
1 to 2 Weeks
- Swelling, bruising, or discomfort may persist but should gradually improve.
- Light activities may be resumed depending on your doctor's advice.
- Attend your first follow-up appointment for progress monitoring.
2 to 4 Weeks
- Begin physical therapy or gentle rehabilitation exercises if mobility was affected.
- Gradually return to daily activities while avoiding strenuous tasks.
- Continue medication if prescribed to manage calcium levels or underlying issues.
4 to 6 Weeks
- Significant improvement in pain and function.
- Many patients can return to most normal activities.
- Continue follow-up visits to ensure proper healing.
6 Weeks and Beyond
- Full recovery is expected for many patients, though this depends on lesion size and location.
- Long-term management may include lifestyle changes and ongoing medical treatment to prevent recurrence.
Benefits of Calcified Lesions Treatment
- Relief from pain and discomfort
- Improved mobility and function
- Prevention of organ damage or complications
- Better management of underlying conditions
- Improved quality of life
Possible Risks of Calcified Lesions
While most patients recover well, risks may include:
- Infection (rare)
- Blood clots (if surgery is performed)
- Recurrence of calcifications
- Organ dysfunction if left untreated
- Complications related to underlying diseases
Calcified Lesions Treatment Cost in India
Calcified lesions are hardened deposits of calcium that can form in blood vessels, the heart, or other tissues, making medical treatment more complex. Managing these lesions often requires specialized procedures like angioplasty with advanced imaging or surgical interventions to restore proper blood flow and prevent complications.
The cost of calcified lesions treatment in India typically ranges from Rs. 1,20,000 to Rs. 3,50,000, depending on factors such as the severity of the condition, the treatment approach (angioplasty, atherectomy, or surgery), hospital facilities, and the patient's overall health condition.
Patient Success Stories
Real experiences from patients who regained their mobility and quality of life
""I went to Medicover for treatment of calcified lesions, and the doctors explained the condition in detail. The procedure was handled smoothly, and I felt much better afterwards.""
""The doctors at Medicover were very supportive during my treatment for calcified lesions. They took the time to answer all my questions, which really reduced my stress.""
""I had been struggling with discomfort due to calcified lesions. At Medicover, the diagnosis was quick, and the treatment was done with care. I am satisfied with the results.""
Frequently Asked Questions
1. What is the recovery time for calcified lesions?
Recovery time depends on the location and treatment method. Mild cases may require no recovery, while treated cases (like surgery or procedures) may take a few weeks to months for full healing.
2. What are calcified lesions in coronary arteries?
Calcified lesions in coronary arteries refer to hardened calcium deposits in the artery walls. These can restrict blood flow and increase the risk of heart disease or heart attacks.
3. What is a calcified lesion in the brain?
A calcified lesion in the brain is a buildup of calcium deposits in brain tissue. It may occur due to infections, old injuries, or certain medical conditions and is often detected through imaging scans.
4. Is calcification dangerous?
Calcification is not always dangerous, but it can be serious depending on where it occurs. In vital organs like the heart or brain, it may affect function and require medical attention.
5. What is a calcified lesion in the heart?
A calcified lesion in the heart typically refers to calcium buildup in the heart valves or coronary arteries, which can affect blood flow and lead to cardiovascular problems.
6. What causes calcification?
Calcification can be caused by aging, inflammation, infections, injury, metabolic disorders, or chronic conditions like kidney disease or atherosclerosis.
7. What is bone calcification treatment?
Treatment depends on the cause and may include medications, physical therapy, lifestyle changes, or surgery in severe cases to manage symptoms and improve mobility.
8. Is brain calcification dangerous?
Brain calcification is not always harmful, but in some cases, it may be linked to neurological symptoms or underlying conditions that require medical evaluation.
9. What are calcified liver lesions?
Calcified liver lesions are calcium deposits in the liver, often resulting from previous infections or benign conditions. Most are harmless, but some cases may need monitoring or further evaluation.
Feeling unwell?
Book Doctor Appointment in 30 Sec